EX-99.2
Published on January 11, 2021
Exhibit 99.2
|
As of December 31, 2020 nasdaq: axgn Corporate presentation |
|
2 This presentation contains “forward-looking” statements as defined in the Private Securities Litigation Reform Act of 1995. These statements are based on management's current expectations or predictions of future conditions, events, or results based on various assumptions and management's estimates of trends and economic factors in the markets in which we are active, as well as our business plans. Words such as “expects,” “anticipates,” “intends,” “plans,” “believes,” “seeks,” “estimates,” “projects,” “forecasts,” “continue,” “may,” “should,” “will,” “goals,” and variations of such words and similar expressions are intended to identify such forward- looking statements. The forward-looking statements may include, without limitation, statements related to the expected impact of COVID-19 on our business, statements regarding product development, product potential, financial performance, sales growth, product adoption, market awareness of our products, data validation, our assessment of our internal controls over financial reporting, our visibility at and sponsorship of conferences and educational events. The forward-looking statements are and will be subject to risks and uncertainties, which may cause actual results to differ materially from those expressed or implied in such forward-looking statements. Forward-looking statements contained in this presentation should be evaluated together with the many uncertainties that affect our business and our market, particularly those discussed under Part I, Item 1A., “Risk Factors,” of our Annual Report on Form 10-K, as amended on Form 10-K/A, for the fiscal year ended December 31, 2019, as well as other risks and cautionary statements set forth in our filings with the U.S. Securities and Exchange Commission. Forward-looking statements are not a guarantee of future performance, and actual results may differ materially from those projected. The forward-looking statements are representative only as of the date they are made and, except as required by applicable law, we assume no responsibility to publicly update or revise any forward- looking statements, whether as a result of new information, future events, changed circumstances, or otherwise. Safe harbor statement revolutionizing the science of nerve repair™ |
|
3 The Axogen platform for nerve repair revolutionizing the science of nerve repair™ |
|
4 The function of nerves Nerves are like wires • Transfer signals across a network • If cut, data cannot be transferred • If crushed, short circuits and data corruption may occur The peripheral nervous system is a vast network from every organ to and from the brain • Sensory • Motor • Autonomic revolutionizing the science of nerve repair™ |
|
Axogen is the preeminent nerve repair company with a foundation for long-term sustainable growth 5 Exclusively focused on peripheral nerve repair across an expanding set of applications addressing large market opportunity Differentiated platform for nerve repair, anchored by Avance® Nerve Graft 10+ years of demonstrated clinical consistency and meaningful recovery outcomes 138 peer-reviewed clinical publications featuring the Axogen product portfolio (as of September 30, 2020) Avance RMAT designation highlights clinical evidence strength and unmet medical need for improved nerve injury treatments Commercial and Professional Education capability to convert experienced surgeons while training the next generation Significant barriers to competitive entry Solid balance sheet provides resources to execute business plan Experienced management team with strong track record of success revolutionizing the science of nerve repair™ |
|
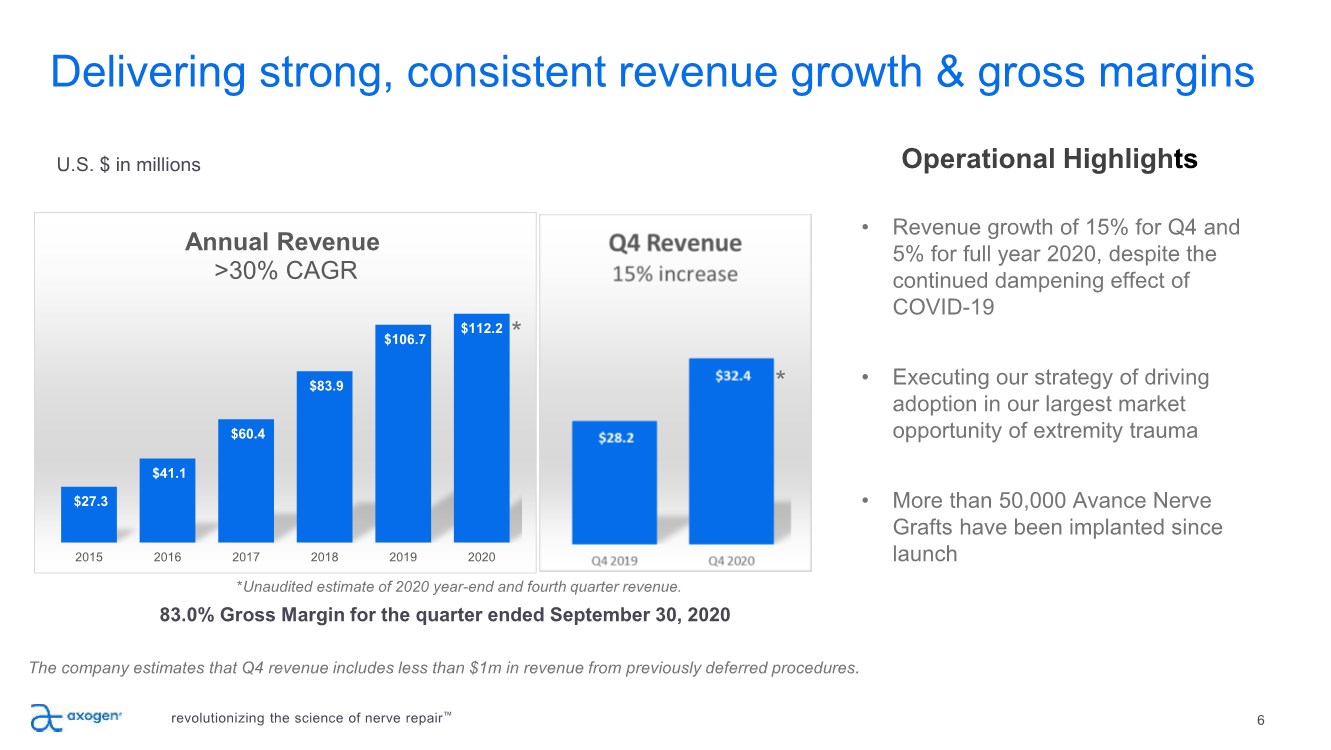
6 83.0% Gross Margin for the quarter ended September 30, 2020 U.S. $ in millions Delivering strong, consistent revenue growth & gross margins revolutionizing the science of nerve repair™ Operational Highlights The company estimates that Q4 revenue includes less than $1m in revenue from previously deferred procedures. • Revenue growth of 15% for Q4 and 5% for full year 2020, despite the continued dampening effect of COVID-19 • Executing our strategy of driving adoption in our largest market opportunity of extremity trauma • More than 50,000 Avance Nerve Grafts have been implanted since launch $27.3 $41.1 $60.4 $83.9 $106.7 $112.2 2015 2016 2017 2018 2019 2020 Annual Revenue >30% CAGR * *Unaudited estimate of 2020 year-end and fourth quarter revenue. * |
|
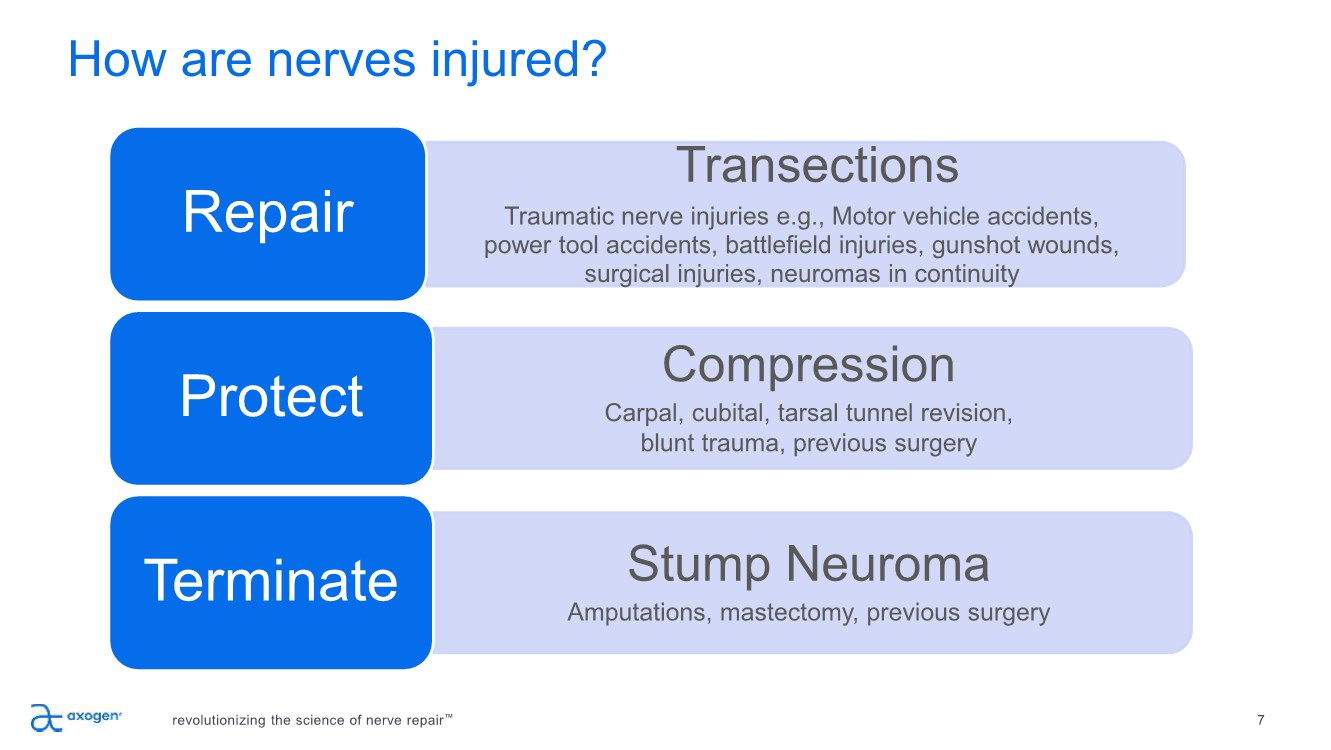
revolutionizing the science of nerve repair™ 7 How are nerves injured? Transections Traumatic nerve injuries e.g., Motor vehicle accidents, power tool accidents, battlefield injuries, gunshot wounds, surgical injuries, neuromas in continuity Repair Compression Carpal, cubital, tarsal tunnel revision, blunt trauma, previous surgery Protect Stump Neuroma Amputations, mastectomy, previous surgery Terminate |
|
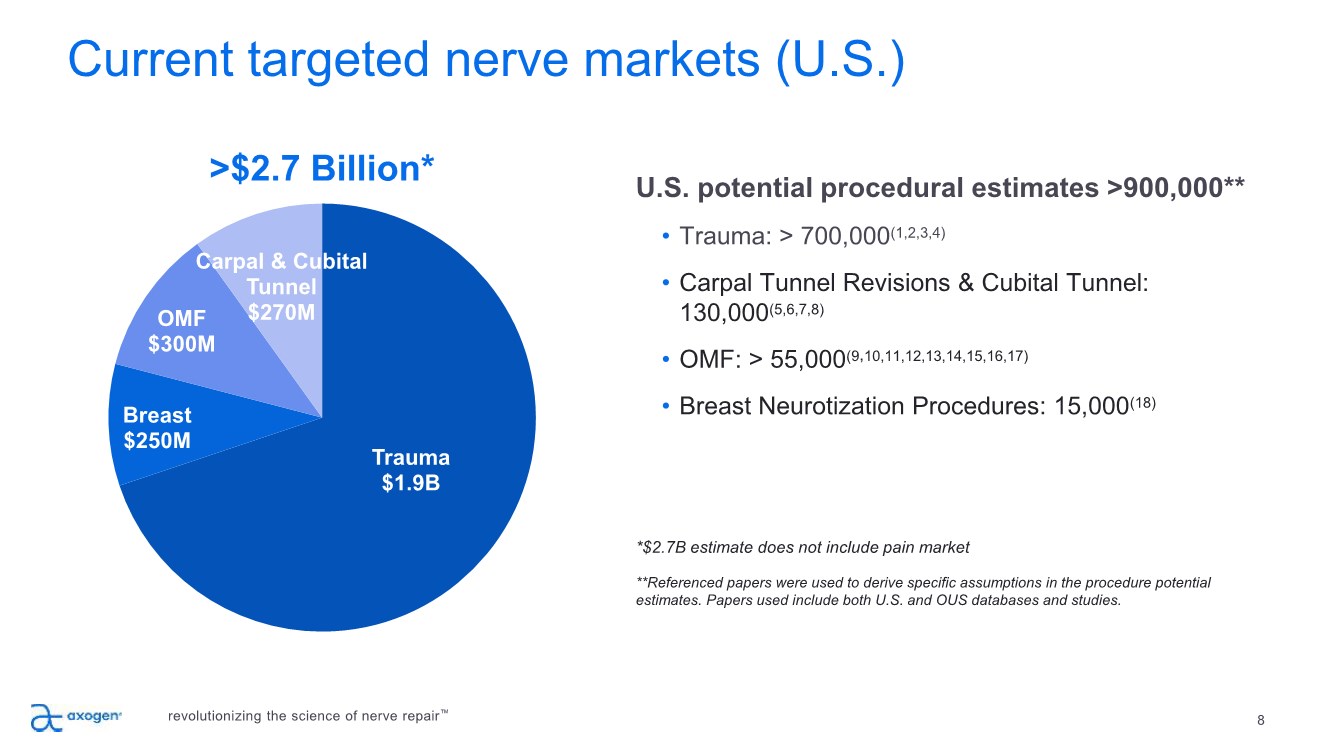
Current targeted nerve markets (U.S.) 8 Trauma $1.9B Breast $250M OMF $300M Carpal & Cubital Tunnel $270M U.S. potential procedural estimates >900,000** • Trauma: > 700,000(1,2,3,4) • Carpal Tunnel Revisions & Cubital Tunnel: 130,000(5,6,7,8) • OMF: > 55,000(9,10,11,12,13,14,15,16,17) • Breast Neurotization Procedures: 15,000(18) *$2.7B estimate does not include pain market **Referenced papers were used to derive specific assumptions in the procedure potential estimates. Papers used include both U.S. and OUS databases and studies. >$2.7 Billion* revolutionizing the science of nerve repair™ |
|
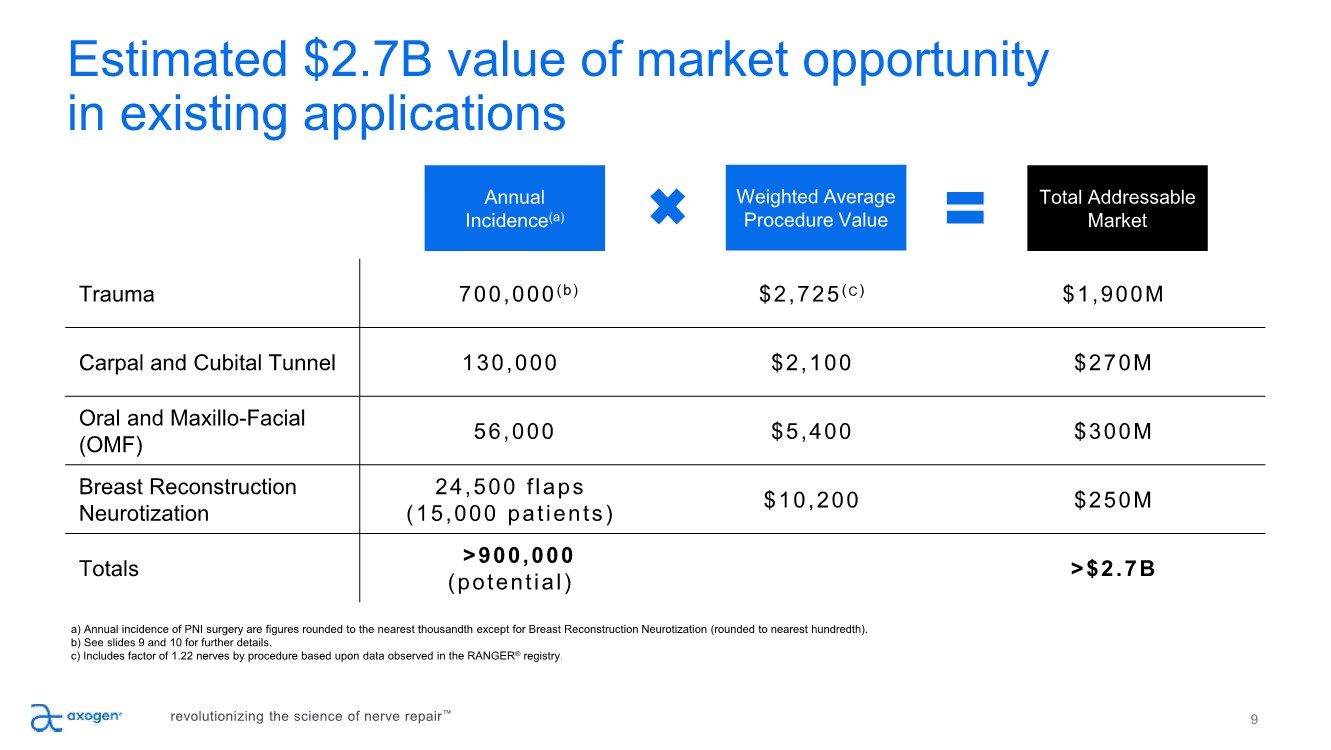
Annual Incidence(a) Weighted Average Procedure Value Total Addressable Market Trauma 700,000(b) $2,725(C) $1,900M Carpal and Cubital Tunnel 130,000 $2,100 $270M Oral and Maxillo-Facial (OMF) 56,000 $5,400 $300M Breast Reconstruction Neurotization 24,500 flaps (15,000 patients) $10,200 $250M Totals >900,000 (potential) >$2.7B a) Annual incidence of PNI surgery are figures rounded to the nearest thousandth except for Breast Reconstruction Neurotization (rounded to nearest hundredth). b) See slides 9 and 10 for further details. c) Includes factor of 1.22 nerves by procedure based upon data observed in the RANGER® registry. 9 Estimated $2.7B value of market opportunity in existing applications revolutionizing the science of nerve repair™ |
|
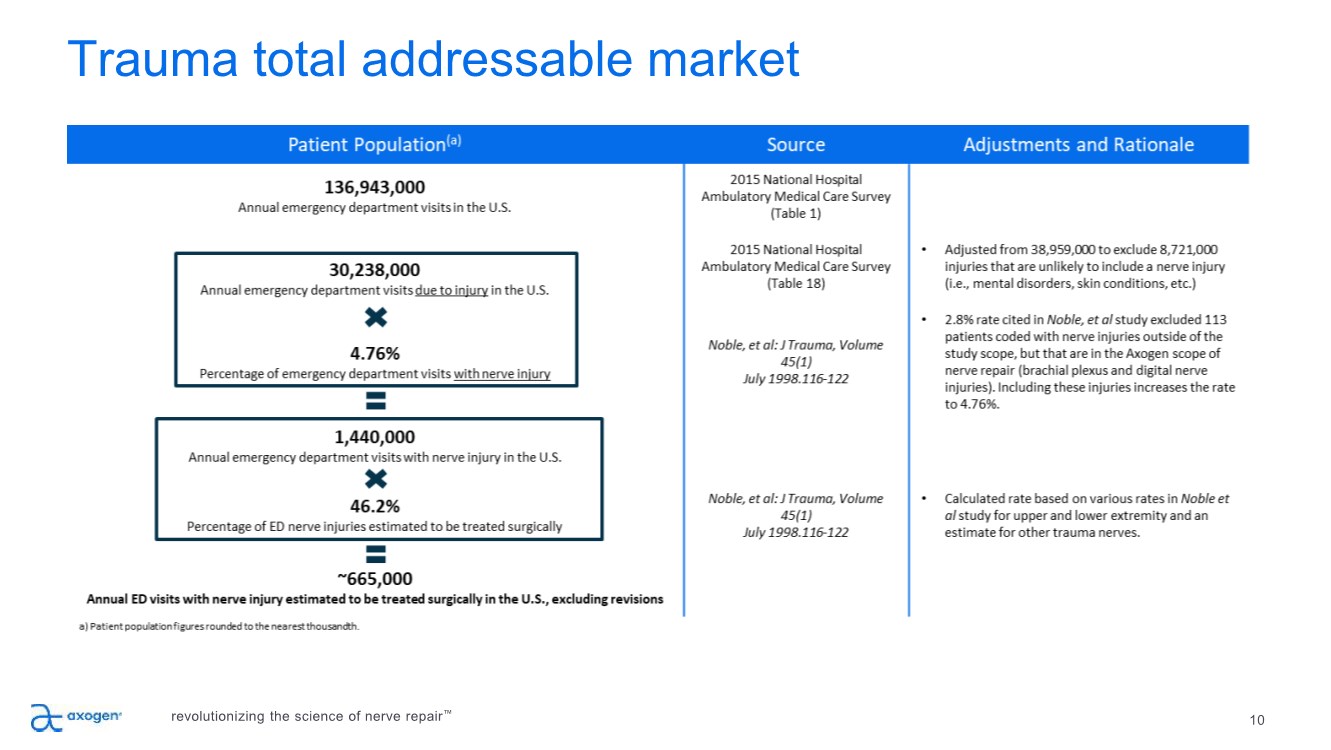
10 Trauma total addressable market revolutionizing the science of nerve repair™ |
|
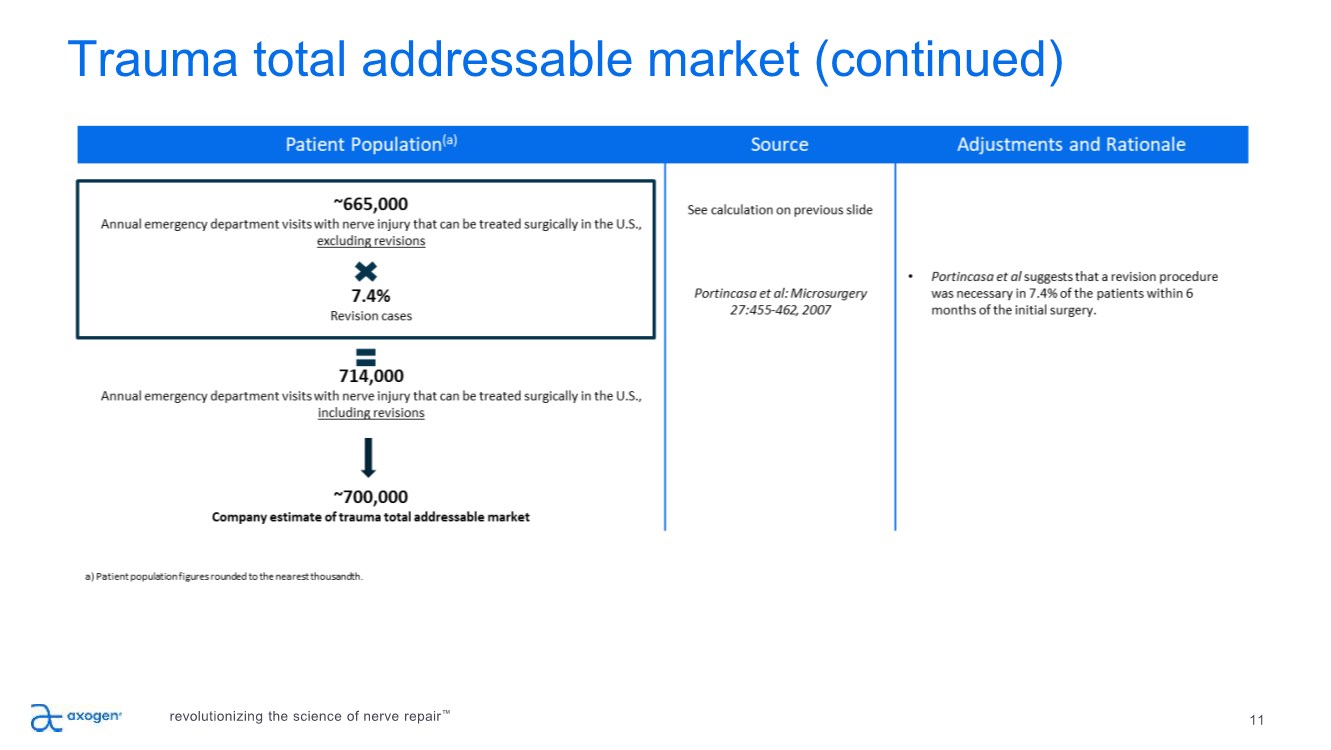
Trauma total addressable market (continued) 11 revolutionizing the science of nerve repair™ |
|
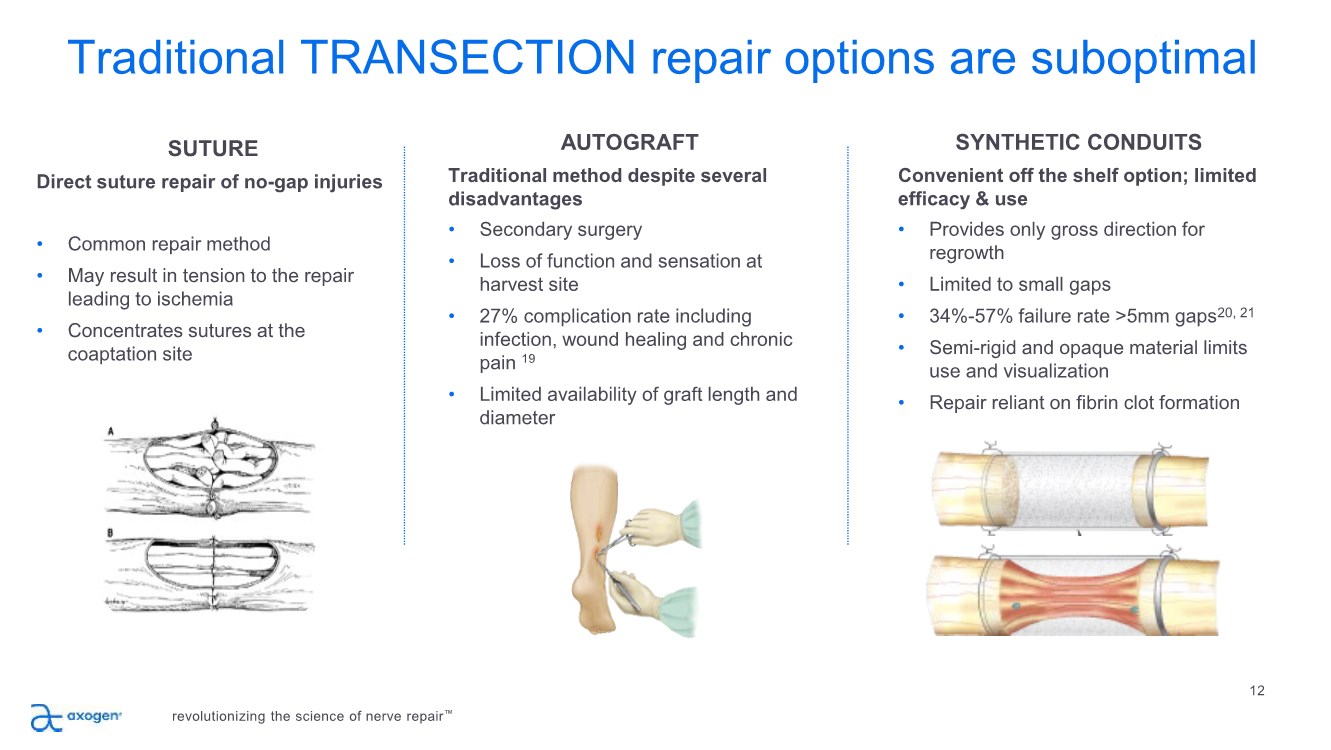
Traditional TRANSECTION repair options are suboptimal 12 SUTURE Direct suture repair of no-gap injuries • Common repair method • May result in tension to the repair leading to ischemia • Concentrates sutures at the coaptation site AUTOGRAFT Traditional method despite several disadvantages • Secondary surgery • Loss of function and sensation at harvest site • 27% complication rate including infection, wound healing and chronic pain 19 • Limited availability of graft length and diameter SYNTHETIC CONDUITS Convenient off the shelf option; limited efficacy & use • Provides only gross direction for regrowth • Limited to small gaps • 34%-57% failure rate >5mm gaps20, 21 • Semi-rigid and opaque material limits use and visualization • Repair reliant on fibrin clot formation revolutionizing the science of nerve repair™ |
|
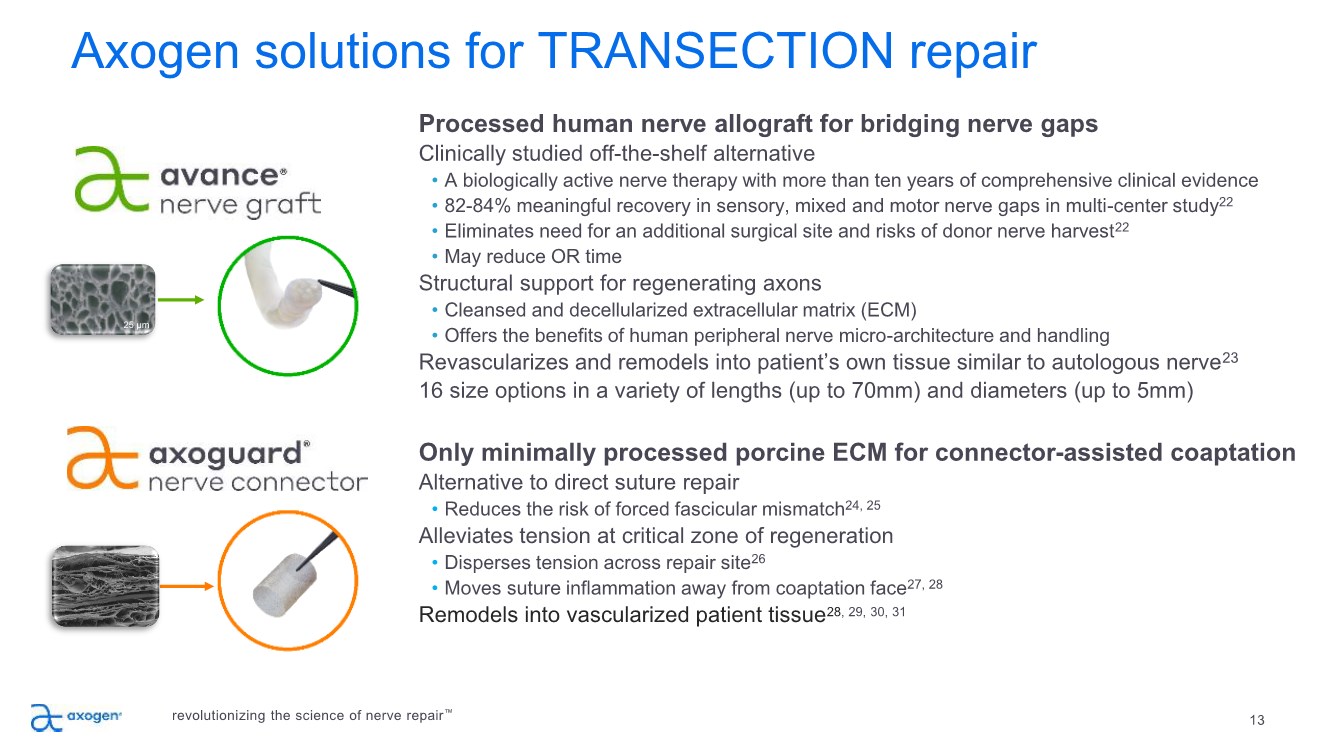
13 25 µm Processed human nerve allograft for bridging nerve gaps Clinically studied off-the-shelf alternative • A biologically active nerve therapy with more than ten years of comprehensive clinical evidence • 82-84% meaningful recovery in sensory, mixed and motor nerve gaps in multi-center study22 • Eliminates need for an additional surgical site and risks of donor nerve harvest22 • May reduce OR time Structural support for regenerating axons • Cleansed and decellularized extracellular matrix (ECM) • Offers the benefits of human peripheral nerve micro-architecture and handling Revascularizes and remodels into patient’s own tissue similar to autologous nerve23 16 size options in a variety of lengths (up to 70mm) and diameters (up to 5mm) Only minimally processed porcine ECM for connector-assisted coaptation Alternative to direct suture repair • Reduces the risk of forced fascicular mismatch24, 25 Alleviates tension at critical zone of regeneration • Disperses tension across repair site26 • Moves suture inflammation away from coaptation face27, 28 Remodels into vascularized patient tissue28, 29, 30, 31 Axogen solutions for TRANSECTION repair revolutionizing the science of nerve repair™ |
|
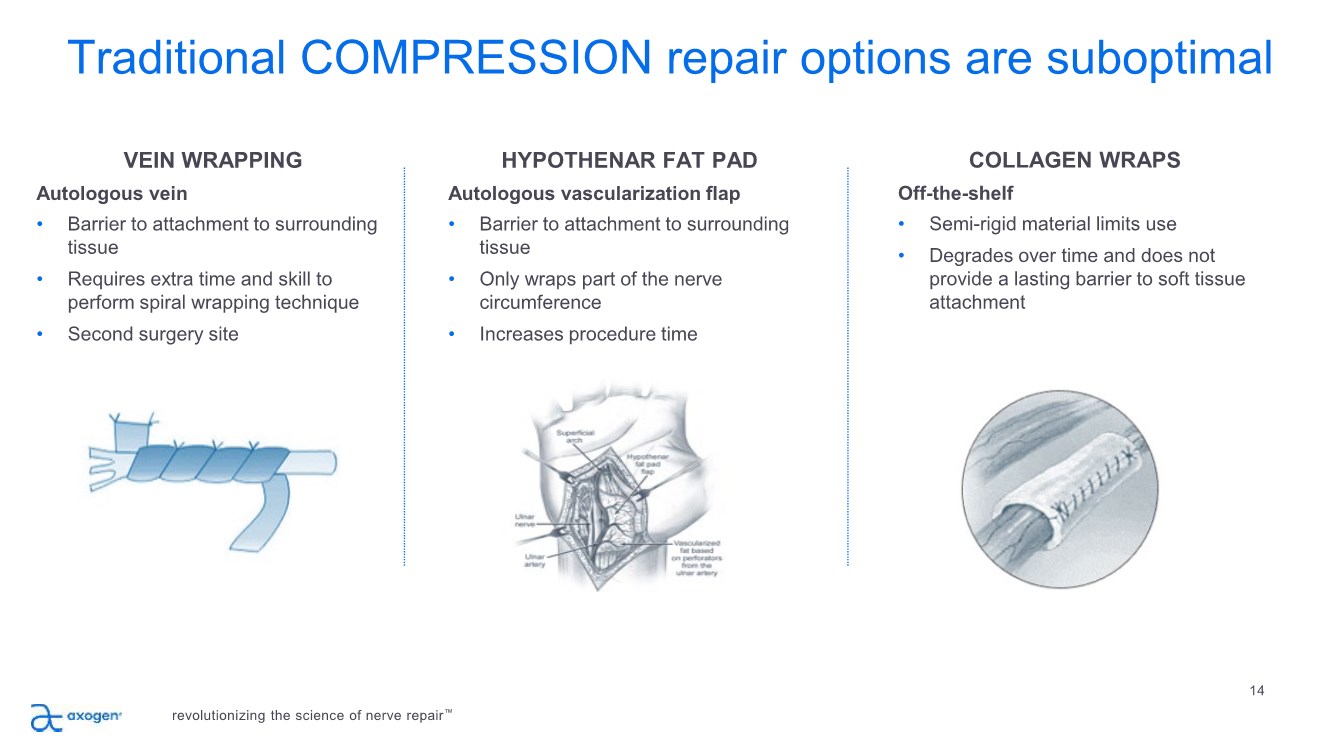
Traditional COMPRESSION repair options are suboptimal 14 VEIN WRAPPING Autologous vein • Barrier to attachment to surrounding tissue • Requires extra time and skill to perform spiral wrapping technique • Second surgery site HYPOTHENAR FAT PAD Autologous vascularization flap • Barrier to attachment to surrounding tissue • Only wraps part of the nerve circumference • Increases procedure time COLLAGEN WRAPS Off-the-shelf • Semi-rigid material limits use • Degrades over time and does not provide a lasting barrier to soft tissue attachment revolutionizing the science of nerve repair™ |
|
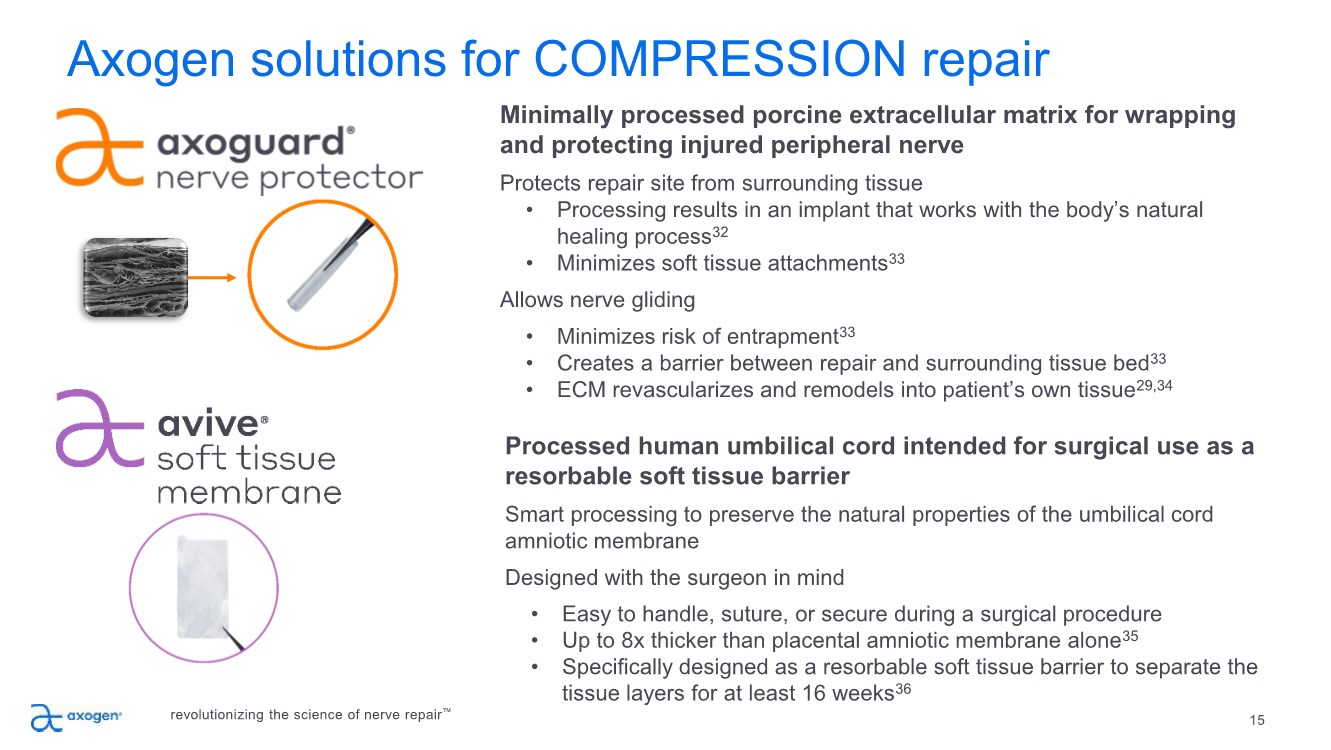
15 Axogen solutions for COMPRESSION repair Minimally processed porcine extracellular matrix for wrapping and protecting injured peripheral nerve Protects repair site from surrounding tissue • Processing results in an implant that works with the body’s natural healing process32 • Minimizes soft tissue attachments33 Allows nerve gliding • Minimizes risk of entrapment33 • Creates a barrier between repair and surrounding tissue bed33 • ECM revascularizes and remodels into patient’s own tissue29,34 revolutionizing the science of nerve repair™ Processed human umbilical cord intended for surgical use as a resorbable soft tissue barrier Smart processing to preserve the natural properties of the umbilical cord amniotic membrane Designed with the surgeon in mind • Easy to handle, suture, or secure during a surgical procedure • Up to 8x thicker than placental amniotic membrane alone35 • Specifically designed as a resorbable soft tissue barrier to separate the tissue layers for at least 16 weeks36 |
|
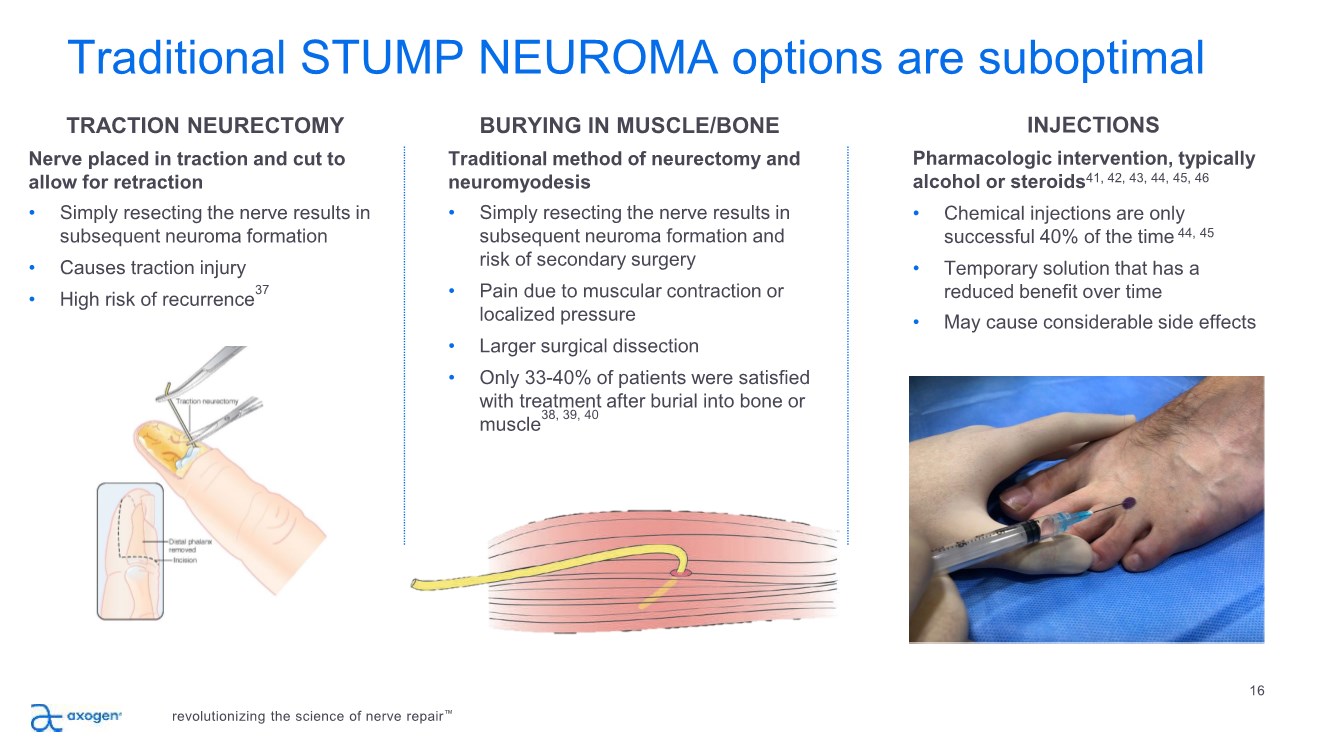
Traditional STUMP NEUROMA options are suboptimal 16 TRACTION NEURECTOMY Nerve placed in traction and cut to allow for retraction • Simply resecting the nerve results in subsequent neuroma formation • Causes traction injury • High risk of recurrence37 BURYING IN MUSCLE/BONE Traditional method of neurectomy and neuromyodesis • Simply resecting the nerve results in subsequent neuroma formation and risk of secondary surgery • Pain due to muscular contraction or localized pressure • Larger surgical dissection • Only 33-40% of patients were satisfied with treatment after burial into bone or muscle38, 39, 40 INJECTIONS Pharmacologic intervention, typically alcohol or steroids41, 42, 43, 44, 45, 46 • Chemical injections are only successful 40% of the time 44, 45 • Temporary solution that has a reduced benefit over time • May cause considerable side effects revolutionizing the science of nerve repair™ |
|
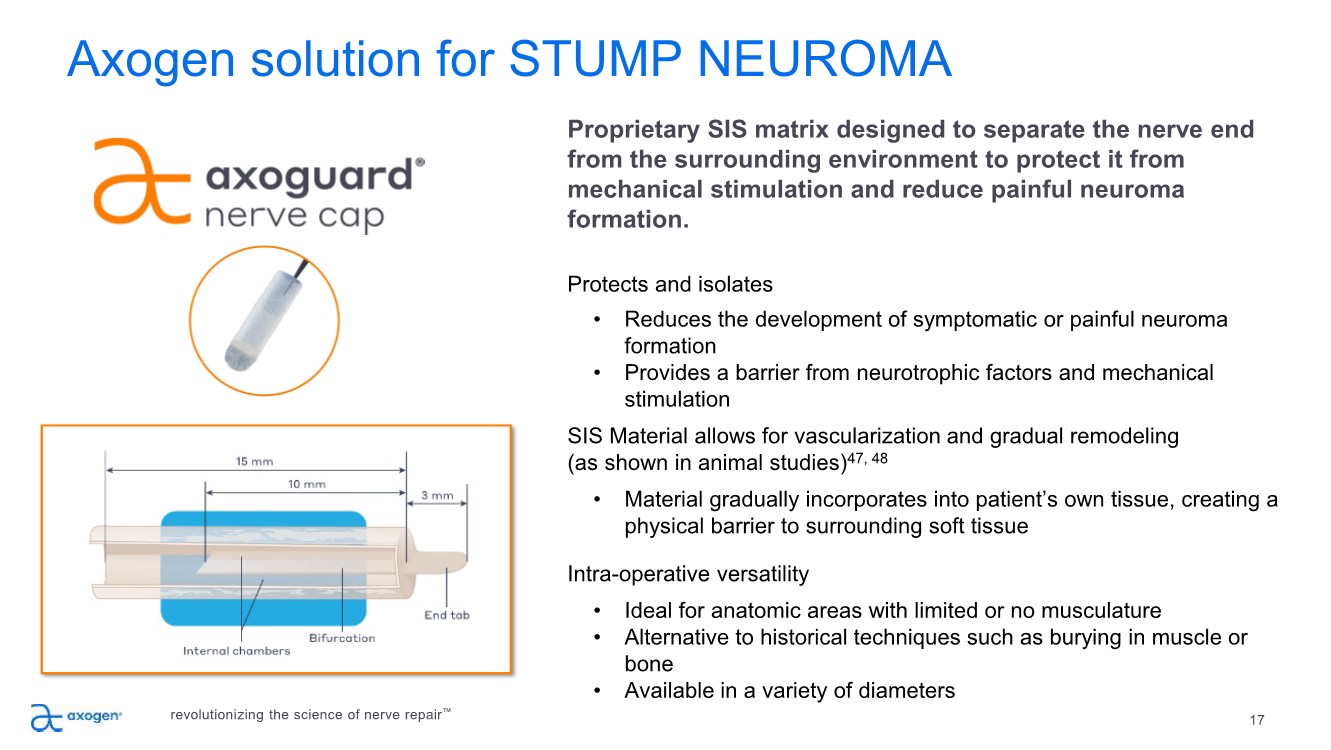
17 Axogen solution for STUMP NEUROMA Proprietary SIS matrix designed to separate the nerve end from the surrounding environment to protect it from mechanical stimulation and reduce painful neuroma formation. Protects and isolates • Reduces the development of symptomatic or painful neuroma formation • Provides a barrier from neurotrophic factors and mechanical stimulation SIS Material allows for vascularization and gradual remodeling (as shown in animal studies)47, 48 • Material gradually incorporates into patient’s own tissue, creating a physical barrier to surrounding soft tissue Intra-operative versatility • Ideal for anatomic areas with limited or no musculature • Alternative to historical techniques such as burying in muscle or bone • Available in a variety of diameters revolutionizing the science of nerve repair™ |
|
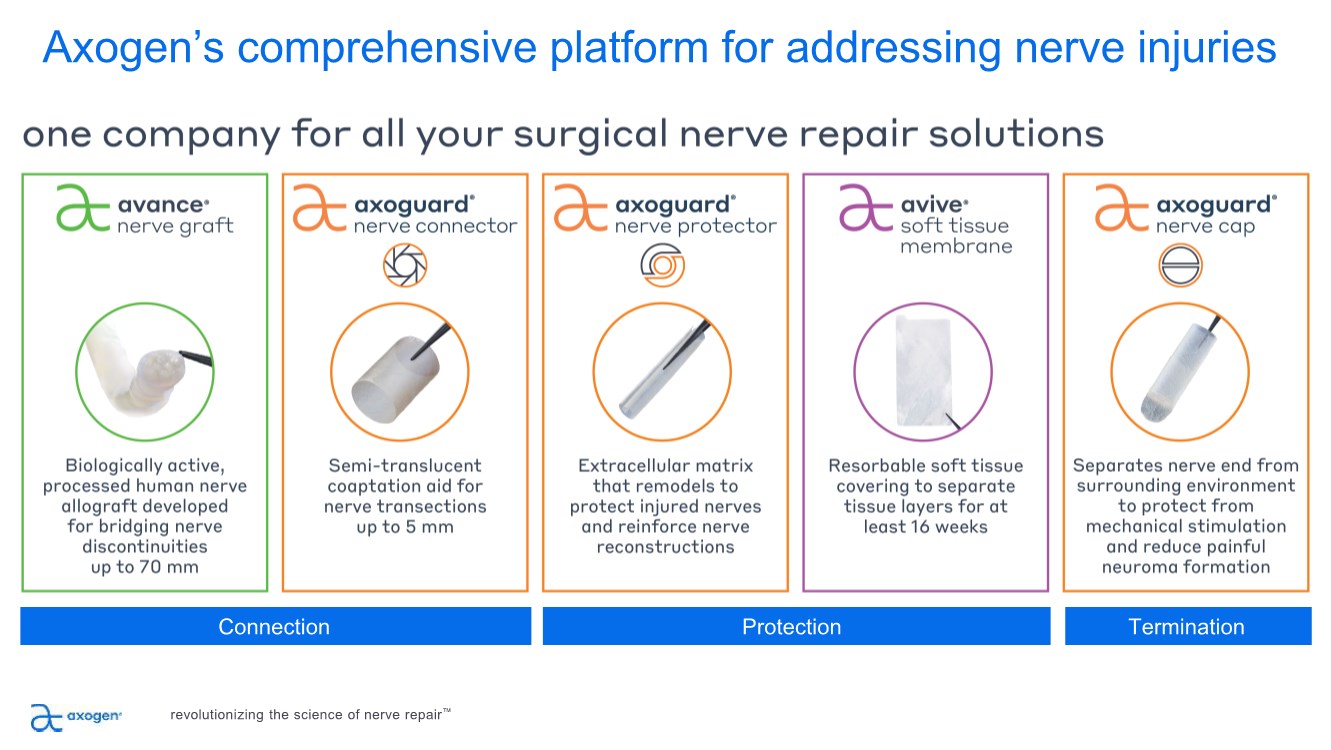
Axogen’s comprehensive platform for addressing nerve injuries Connection Protection Termination revolutionizing the science of nerve repair™ |
|
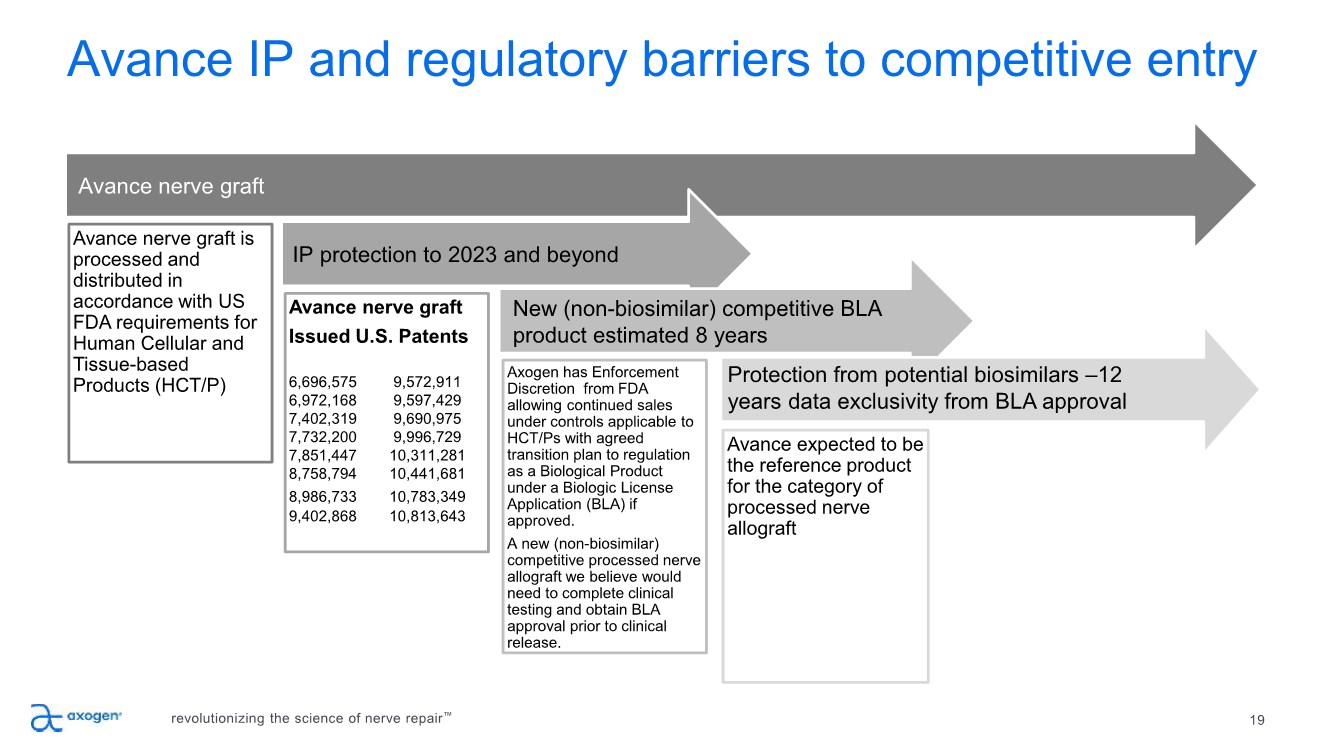
19 Avance IP and regulatory barriers to competitive entry Avance nerve graft is processed and distributed in accordance with US FDA requirements for Human Cellular and Tissue-based Products (HCT/P) Avance nerve graft Issued U.S. Patents 6,696,575 9,572,911 6,972,168 9,597,429 7,402,319 9,690,975 7,732,200 9,996,729 7,851,447 10,311,281 8,758,794 10,441,681 8,986,733 10,783,349 9,402,868 10,813,643 Axogen has Enforcement Discretion from FDA allowing continued sales under controls applicable to HCT/Ps with agreed transition plan to regulation as a Biological Product under a Biologic License Application (BLA) if approved. A new (non-biosimilar) competitive processed nerve allograft we believe would need to complete clinical testing and obtain BLA approval prior to clinical release. Avance expected to be the reference product for the category of processed nerve allograft Avance nerve graft IP protection to 2023 and beyond New (non-biosimilar) competitive BLA product estimated 8 years Protection from potential biosimilars –12 years data exclusivity from BLA approval revolutionizing the science of nerve repair™ |
|
Unique Avance technology creates barriers to competitive entry revolutionizing the science of nerve repair™ 20 Progress toward Biologics License Application (BLA) for Avance nerve graft • Received Regenerative Medicine Advanced Therapy (RMAT) designation for Avance Nerve Graft in September 2018 – Highlights strength of clinical evidence and the unmet medical need for improved therapies to treat nerve injuries • RECON target enrollment of 220 subjects was reached in July 2020 – Prospective randomized controlled double-blinded study compares Avance Nerve Graft to synthetic conduits in digital injuries – The study protocol requires a one-year follow-up assessment with an allowance for an additional three-month visit window completing in October 2021 – Preliminary study data report expected in Q2 2022 – Expect to file BLA in 2023 • Expected protection from potential biosimilars – 12-year data exclusivity from date of BLA approval • Building a new 70,000 square foot, state-of-the-art biologics processing facility – Facility being built to cGMP standards under 21 CFR Part 210/211 regulations – Supports long term capacity expansion – Anticipate restarting construction of facility in Q1 2021, after temporary suspension as part of COVID-19 cost mitigation initiative, and transition of tissue processing by late 2022 |
|
21 Market development strategy Build Market Awareness Educate Surgeons, Develop Advocates Grow Body of Clinical Evidence Execute Sales Plan Expand Product Pipeline + Applications revolutionizing the science of nerve repair™ |
|
22 Focus on building awareness among clinicians and patients Build Market Awareness • Increased multi-channel engagement with clinicians and patients • Continuing clinical conference participation virtually • Ongoing patient ambassador program • Garnering positive media attention • Growing social media presence revolutionizing the science of nerve repair™ |
|
23 PILLAR 2 Emphasis on education Build Market Awareness Educate Surgeons, Develop Advocates • Converted national education programs to virtual platforms • Providing customized multimodal learning programs to specific surgeon cohorts for advanced learning • Interactive webinar series underway covering the principles of nerve repair • Trained three-quarters of all hand and micro-surgery fellows in 2020 revolutionizing the science of nerve repair™ |
|
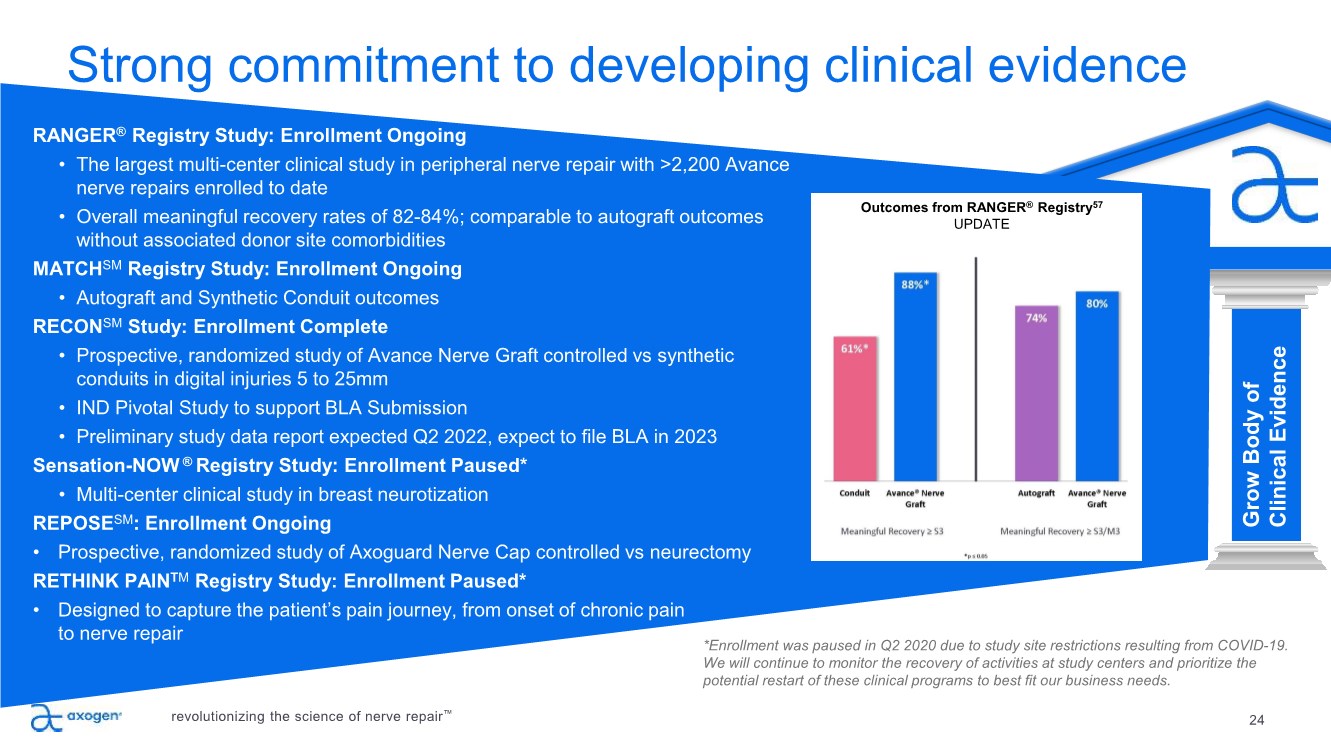
24 PILLAR 3 Strong commitment to developing clinical evidence Build Market Awareness Educate Surgeons, Develop Advocates Grow Body of Clinical Evidence RANGER® Registry Study: Enrollment Ongoing • The largest multi-center clinical study in peripheral nerve repair with >2,200 Avance nerve repairs enrolled to date • Overall meaningful recovery rates of 82-84%; comparable to autograft outcomes without associated donor site comorbidities MATCHSM Registry Study: Enrollment Ongoing • Autograft and Synthetic Conduit outcomes RECONSM Study: Enrollment Complete • Prospective, randomized study of Avance Nerve Graft controlled vs synthetic conduits in digital injuries 5 to 25mm • IND Pivotal Study to support BLA Submission • Preliminary study data report expected Q2 2022, expect to file BLA in 2023 Sensation-NOW ® Registry Study: Enrollment Paused* • Multi-center clinical study in breast neurotization REPOSESM: Enrollment Ongoing • Prospective, randomized study of Axoguard Nerve Cap controlled vs neurectomy RETHINK PAINTM Registry Study: Enrollment Paused* • Designed to capture the patient’s pain journey, from onset of chronic pain to nerve repair revolutionizing the science of nerve repair™ *Enrollment was paused in Q2 2020 due to study site restrictions resulting from COVID-19. We will continue to monitor the recovery of activities at study centers and prioritize the potential restart of these clinical programs to best fit our business needs. Outcomes from RANGER® Registry57 UPDATE |
|
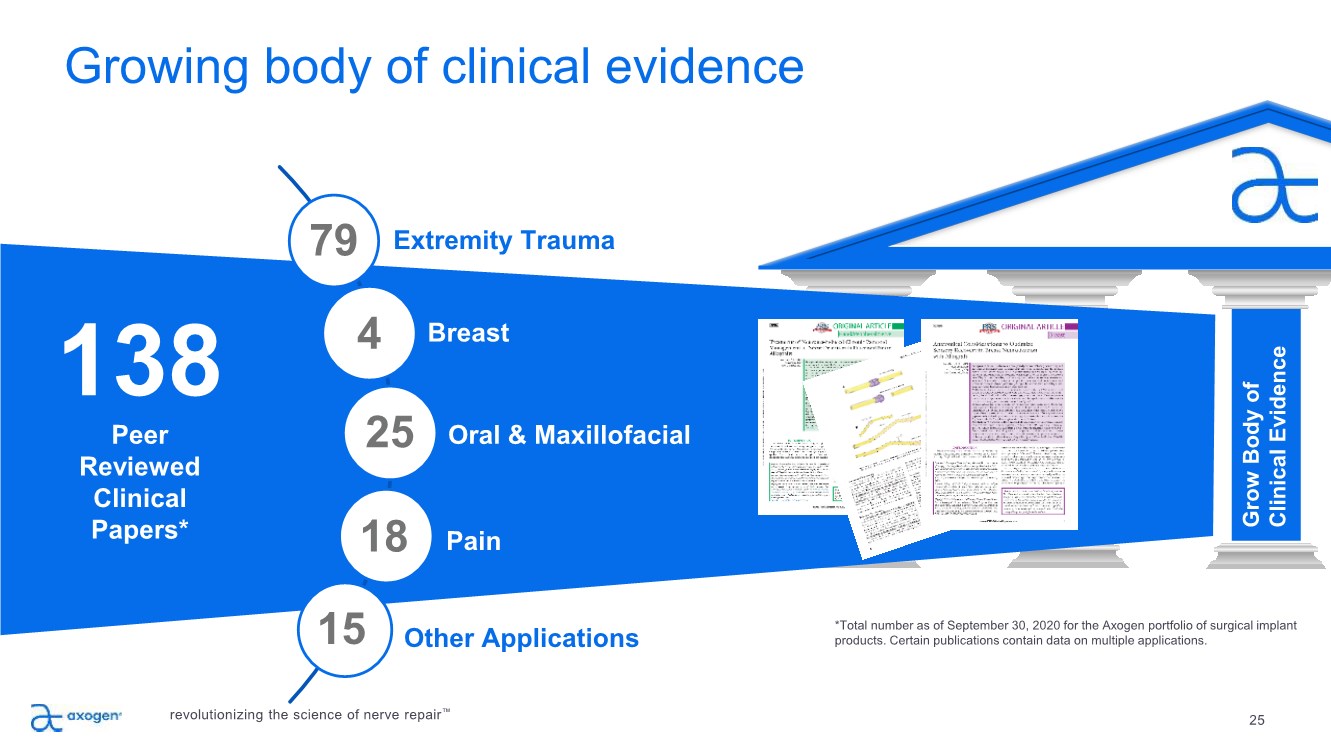
25 PILLAR 3 *Total number as of September 30, 2020 for the Axogen portfolio of surgical implant products. Certain publications contain data on multiple applications. Growing body of clinical evidence Build Market Awareness Educate Surgeons, Develop Advocates Grow Body of Clinical Evidence 138 Peer Reviewed Clinical Papers* Extremity Trauma Breast Oral & Maxillofacial Other Applications 79 4 Pain 25 18 15 revolutionizing the science of nerve repair™ |
|
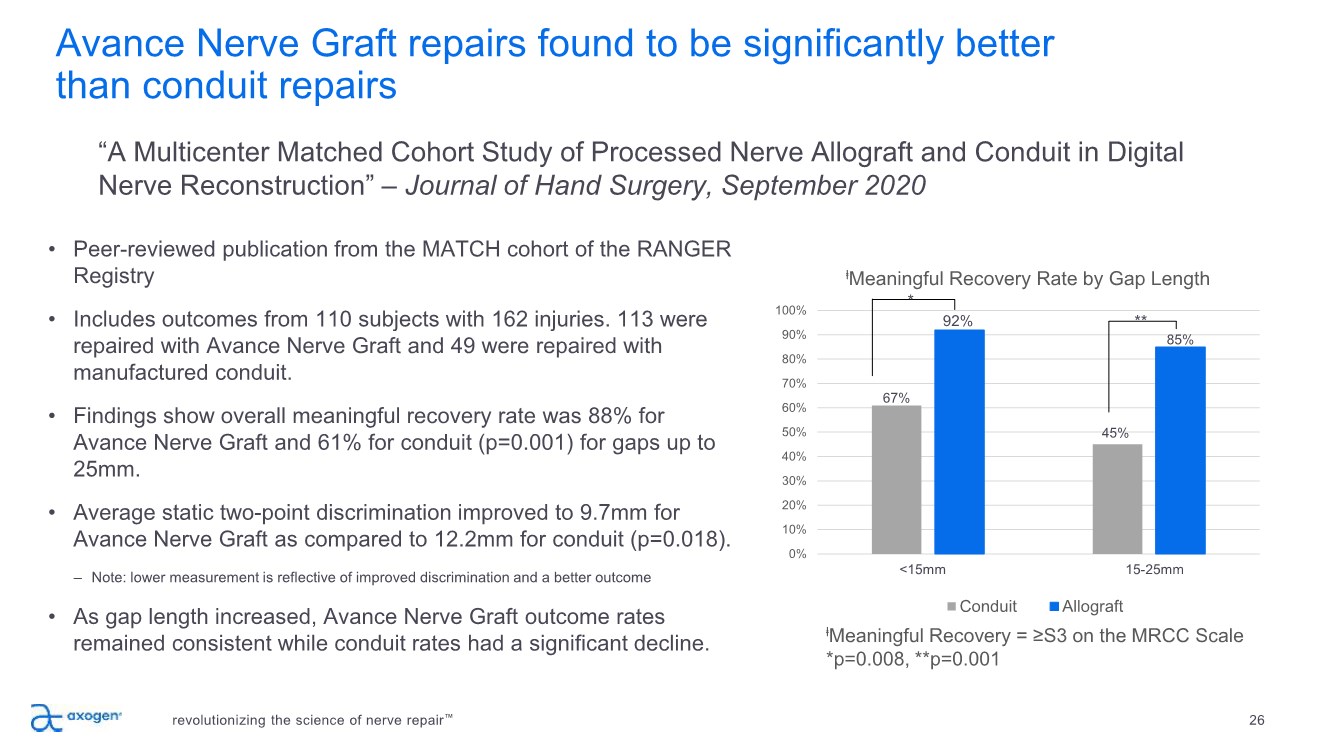
Avance Nerve Graft repairs found to be significantly better than conduit repairs revolutionizing the science of nerve repair™ 26 • Peer-reviewed publication from the MATCH cohort of the RANGER Registry • Includes outcomes from 110 subjects with 162 injuries. 113 were repaired with Avance Nerve Graft and 49 were repaired with manufactured conduit. • Findings show overall meaningful recovery rate was 88% for Avance Nerve Graft and 61% for conduit (p=0.001) for gaps up to 25mm. • Average static two-point discrimination improved to 9.7mm for Avance Nerve Graft as compared to 12.2mm for conduit (p=0.018). – Note: lower measurement is reflective of improved discrimination and a better outcome • As gap length increased, Avance Nerve Graft outcome rates remained consistent while conduit rates had a significant decline. “A Multicenter Matched Cohort Study of Processed Nerve Allograft and Conduit in Digital Nerve Reconstruction” – Journal of Hand Surgery, September 2020 ⱡMeaningful Recovery = ≥S3 on the MRCC Scale *p=0.008, **p=0.001 0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100% ⱡMeaningful Recovery Rate by Gap Length Conduit Allograft <15mm 15-25mm 67% 92% 45% 85% * ** |
|
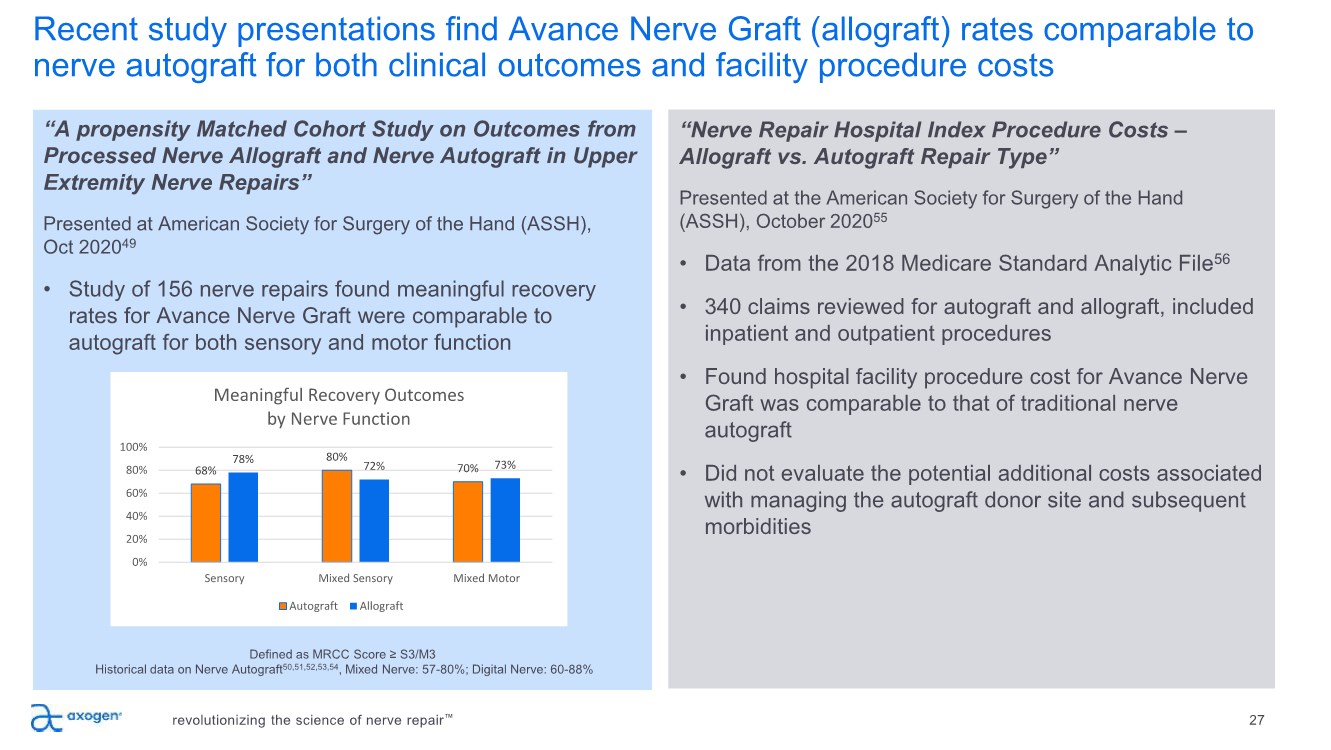
Recent study presentations find Avance Nerve Graft (allograft) rates comparable to nerve autograft for both clinical outcomes and facility procedure costs revolutionizing the science of nerve repair™ 27 “A propensity Matched Cohort Study on Outcomes from Processed Nerve Allograft and Nerve Autograft in Upper Extremity Nerve Repairs” Presented at American Society for Surgery of the Hand (ASSH), Oct 202049 • Study of 156 nerve repairs found meaningful recovery rates for Avance Nerve Graft were comparable to autograft for both sensory and motor function Defined as MRCC Score ≥ S3/M3 Historical data on Nerve Autograft50,51,52,53,54, Mixed Nerve: 57-80%; Digital Nerve: 60-88% “Nerve Repair Hospital Index Procedure Costs – Allograft vs. Autograft Repair Type” Presented at the American Society for Surgery of the Hand (ASSH), October 202055 • Data from the 2018 Medicare Standard Analytic File56 • 340 claims reviewed for autograft and allograft, included inpatient and outpatient procedures • Found hospital facility procedure cost for Avance Nerve Graft was comparable to that of traditional nerve autograft • Did not evaluate the potential additional costs associated with managing the autograft donor site and subsequent morbidities 68% 80% 70% 78% 72% 73% 0% 20% 40% 60% 80% 100% Sensory Mixed Sensory Mixed Motor Meaningful Recovery Outcomes by Nerve Function Autograft Allograft |
|
28 PILLAR 4 Focused sales execution, increasing market penetration Build Market Awareness Educate Surgeons, Develop Advocates Grow Body of Clinical Evidence Execute Sales Plan Sales execution focused on driving results • Continue driving penetration in active accounts and developing new active accounts • 5,100 potential U.S. accounts perform nerve repair • 893 active accounts as of December 31, 2020, up 12% YoY o Top 10% of active accounts represent approximately 35% of total revenue Expanded sales reach • U.S. direct sales team o 111 direct sales professionals at end of Q4 2020 • Supplemented by independent agencies • Revenue from direct sales channel represented approximately 87% of total revenue in Q4 revolutionizing the science of nerve repair™ |
|
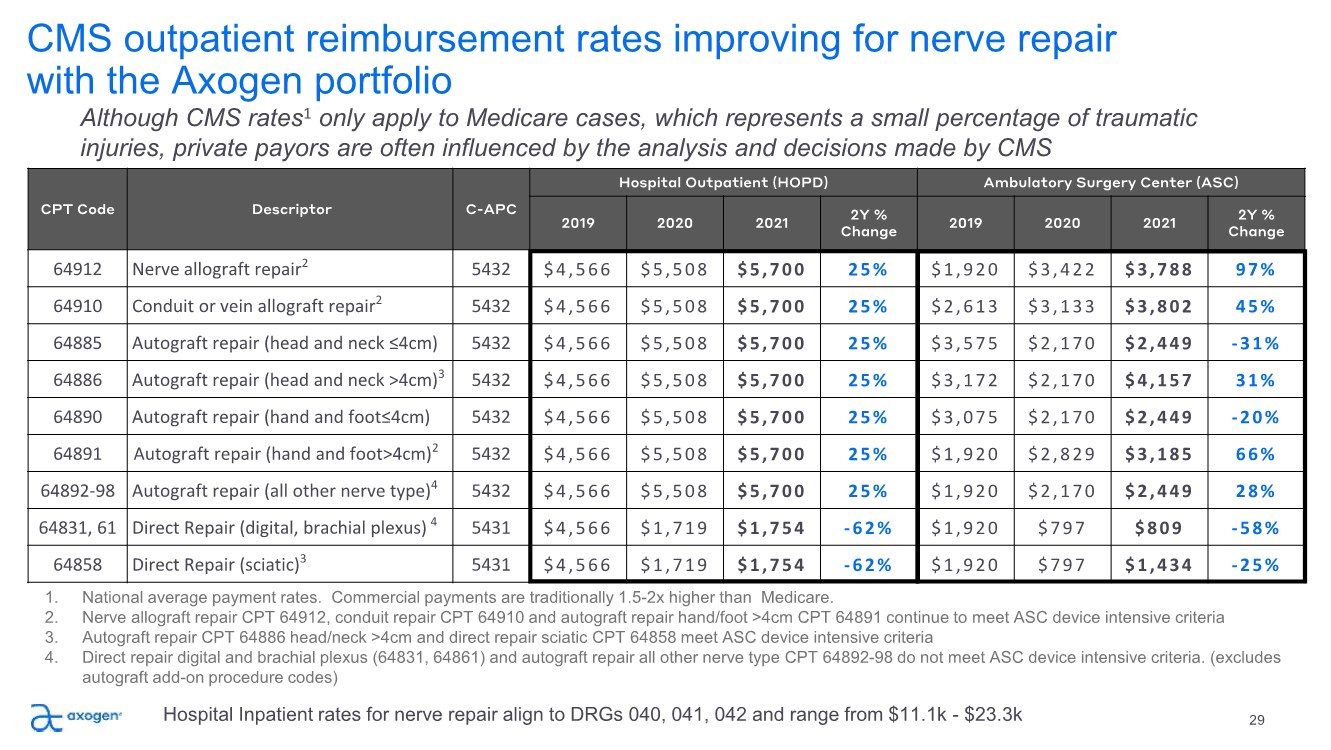
CPT Code Descriptor C-APC Hospital Outpatient (HOPD) Ambulatory Surgery Center (ASC) 2019 2020 2021 2Y % Change 2019 2020 2021 2Y % Change 64912 Nerve allograft repair2 5432 $4,566 $5,508 $5,700 25% $1,920 $3,422 $3,788 97% 64910 Conduit or vein allograft repair2 5432 $4,566 $5,508 $5,700 25% $2,613 $3,133 $3,802 45% 64885 Autograft repair (head and neck ≤4cm) 5432 $4,566 $5,508 $5,700 25% $3,575 $2,170 $2,449 -31% 64886 Autograft repair (head and neck >4cm)3 5432 $4,566 $5,508 $5,700 25% $3,172 $2,170 $4,157 31% 64890 Autograft repair (hand and foot≤4cm) 5432 $4,566 $5,508 $5,700 25% $3,075 $2,170 $2,449 -20% 64891 Autograft repair (hand and foot>4cm)2 5432 $4,566 $5,508 $5,700 25% $1,920 $2,829 $3,185 66% 64892-98 Autograft repair (all other nerve type)4 5432 $4,566 $5,508 $5,700 25% $1,920 $2,170 $2,449 28% 64831, 61 Direct Repair (digital, brachial plexus) 4 5431 $4,566 $1,719 $1,754 -62% $1,920 $797 $809 -58% 64858 Direct Repair (sciatic)3 5431 $4,566 $1,719 $1,754 -62% $1,920 $797 $1,434 -25% CMS outpatient reimbursement rates improving for nerve repair with the Axogen portfolio 29 Although CMS rates1 only apply to Medicare cases, which represents a small percentage of traumatic injuries, private payors are often influenced by the analysis and decisions made by CMS 1. National average payment rates. Commercial payments are traditionally 1.5-2x higher than Medicare. 2. Nerve allograft repair CPT 64912, conduit repair CPT 64910 and autograft repair hand/foot >4cm CPT 64891 continue to meet ASC device intensive criteria 3. Autograft repair CPT 64886 head/neck >4cm and direct repair sciatic CPT 64858 meet ASC device intensive criteria 4. Direct repair digital and brachial plexus (64831, 64861) and autograft repair all other nerve type CPT 64892-98 do not meet ASC device intensive criteria. (excludes autograft add-on procedure codes) Hospital Inpatient rates for nerve repair align to DRGs 040, 041, 042 and range from $11.1k - $23.3k |
|
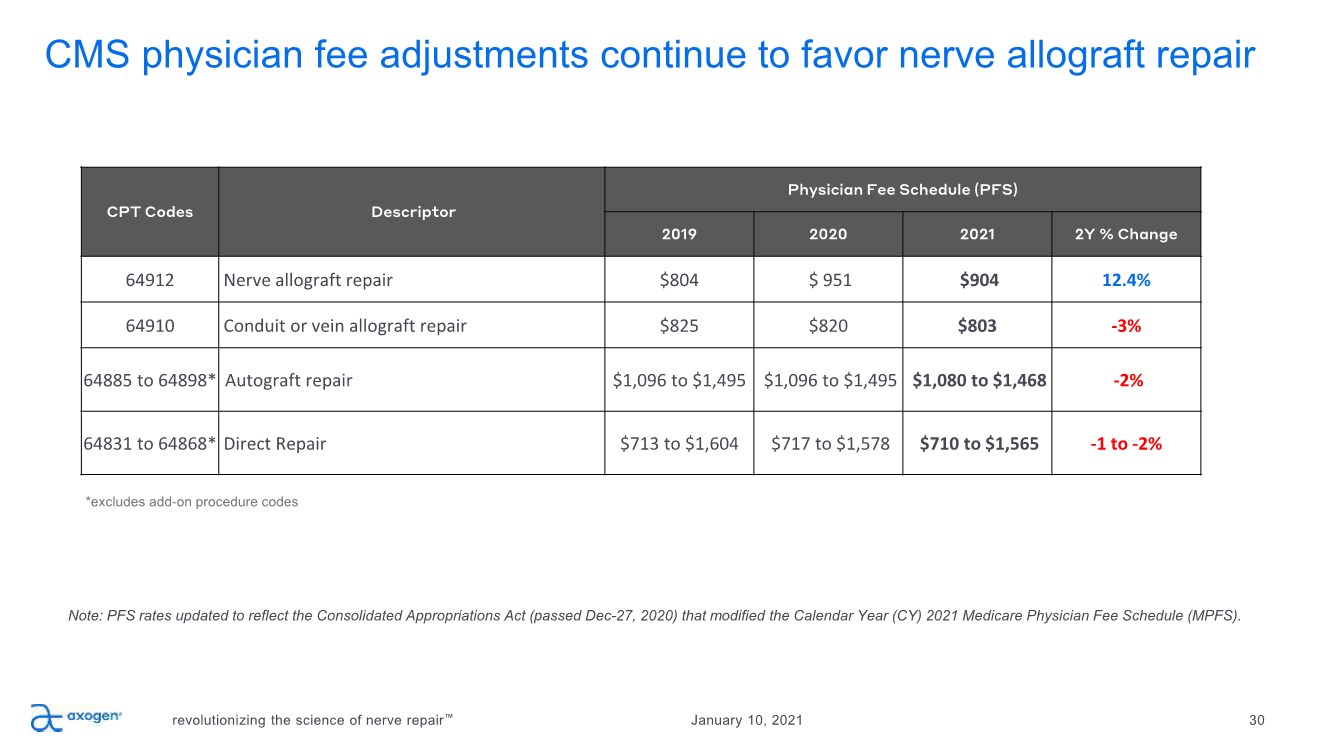
CMS physician fee adjustments continue to favor nerve allograft repair revolutionizing the science of nerve repair™ 30 January 10, 2021 Note: PFS rates updated to reflect the Consolidated Appropriations Act (passed Dec-27, 2020) that modified the Calendar Year (CY) 2021 Medicare Physician Fee Schedule (MPFS). CPT Codes Descriptor Physician Fee Schedule (PFS) 2019 2020 2021 2Y % Change 64912 Nerve allograft repair $804 $ 951 $904 12.4% 64910 Conduit or vein allograft repair $825 $820 $803 -3% 64885 to 64898* Autograft repair $1,096 to $1,495 $1,096 to $1,495 $1,080 to $1,468 -2% 64831 to 64868* Direct Repair $713 to $1,604 $717 to $1,578 $710 to $1,565 -1 to -2% *excludes add-on procedure codes |
|
31 PILLAR 5 Expand the opportunity in nerve repair Build Market Awareness Educate Surgeons, Develop Advocates Grow Body of Clinical Evidence Execute Sales Plan Expand Product Pipeline + Applications International Expansion Product Pipeline Future Market Development Market Expansion Core Business revolutionizing the science of nerve repair™ |
|
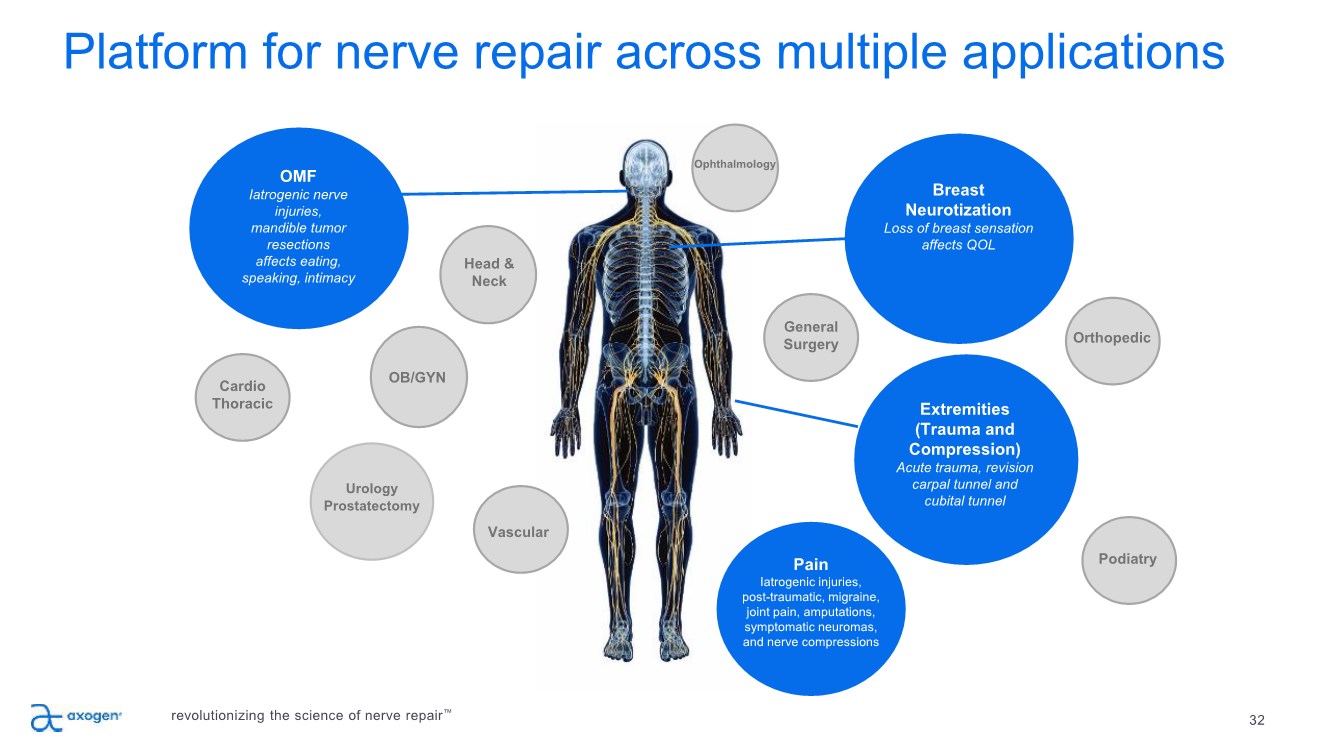
32 Platform for nerve repair across multiple applications Breast Neurotization Loss of breast sensation affects QOL Urology Prostatectomy OMF Iatrogenic nerve injuries, mandible tumor resections affects eating, speaking, intimacy Extremities (Trauma and Compression) Acute trauma, revision carpal tunnel and cubital tunnel Head & Neck OB/GYN General Surgery Cardio Thoracic Orthopedic Podiatry revolutionizing the science of nerve repair™ Vascular Pain Iatrogenic injuries, post-traumatic, migraine, joint pain, amputations, symptomatic neuromas, and nerve compressions Ophthalmology |
|
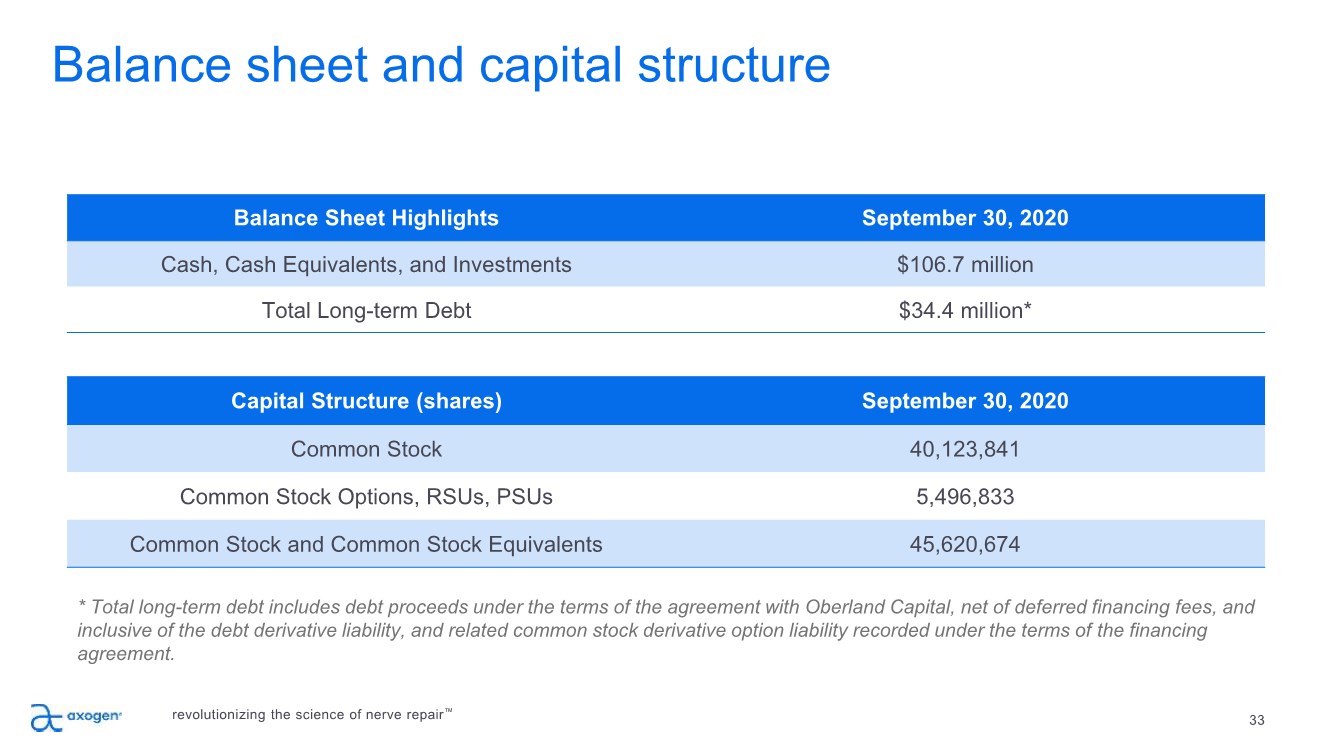
33 Balance Sheet Highlights September 30, 2020 Cash, Cash Equivalents, and Investments $106.7 million Total Long-term Debt $34.4 million* Capital Structure (shares) September 30, 2020 Common Stock 40,123,841 Common Stock Options, RSUs, PSUs 5,496,833 Common Stock and Common Stock Equivalents 45,620,674 Balance sheet and capital structure revolutionizing the science of nerve repair™ * Total long-term debt includes debt proceeds under the terms of the agreement with Oberland Capital, net of deferred financing fees, and inclusive of the debt derivative liability, and related common stock derivative option liability recorded under the terms of the financing agreement. |
|
Executive team 34 Karen Zaderej Chairman, CEO, & President J&J (Ethicon) Peter J. Mariani Chief Financial Officer Guidant, Lensar, Hansen Erick DeVinney VP, Clinical & Translational Sciences Angiotech, PRA Intl Mike Donovan VP, Operations Zimmer Brad Ottinger General Counsel, Chief Compliance Officer MicroPort Orthopedics Eric A. Sandberg Chief Commercial Officer Guidant Ivica Ducic, M.D., Ph.D. Medical Director Washington Nerve Institute Angelo Scopelianos, Ph.D. Chief Research & Development Officer J&J Isabelle Billet Chief Strategy & Business Development Officer J&J, C.R. Bard, Cardinal Maria Martinez Chief Human Resources Officer HSNi, Bausch + Lomb Mark Friedman, Ph.D. VP, Regulatory & QA AtriCure, Enable Medical revolutionizing the science of nerve repair™ |
|
Axogen is the preeminent nerve repair company with a foundation for long-term sustainable growth 35 Exclusively focused on peripheral nerve repair across an expanding set of applications addressing large market opportunity Differentiated platform for nerve repair, anchored by Avance® Nerve Graft 10+ years of demonstrated clinical consistency and meaningful recovery outcomes 138 peer-reviewed clinical publications featuring the Axogen product portfolio (as of September 30, 2020) Avance RMAT designation highlights clinical evidence strength and unmet medical need for improved nerve injury treatments Commercial and Professional Education capability to convert experienced surgeons while training the next generation Significant barriers to competitive entry Solid balance sheet provides resources to execute business plan Experienced management team with strong track record of success revolutionizing the science of nerve repair™ |
|
nasdaq: axgn Deloitte Technology Fast 500: 2014, 2015, 2016, 2017, 2018, 2019 Russell 2000 Index: June 2016 DecisionWise Intl Employee Engagement Best Practices Award Winner: 2018 36 revolutionizing the science of nerve repair™ |
|
37 Footnotes 1. National Hospital Ambulatory Medical Care Survey: 2015 Emergency Department Summary Tables – Table 18. https://www.cdc.gov/nchs/data/nhamcs/web_tables/2015_ed_web_tables.pdf 2. Noble, et al.. Analysis of Upper and Lower Extremity Peripheral Nerve Injuries in a Population of Patients with Multiple Injuries. J Trauma. 1998; 45(1): 116-122. 3. Uzun, et al., Traumatic peripheral nerve injuries: demographic and electrophysiologic findings of 802 patients from a developing country. J Clin Neuromusc Dis. 2006; 7(3): 97–103. 4. Portincasa, et al. Microsurgical treatment of injury to peripheral nerves in upper and lower limbs: a critical review of the last 8 years. Microsurgery. 2007; 27(5): 455–462. 5. Medicare National HCPS Aggregate Summary Table CY2016. https://data.cms.gov/Medicare-Physician-Supplier/Medicare-National-HCPCS-Aggregate-Summary-Table-CY/jtra-d83c/data 6. Sotereanos, et al. Vein wrapping for the treatment of recurrent carpal tunnel syndrome. Tech Hand Up Extrem Surg.1997; 1(1):35-40. 7. Seradge, et al. Cubital tunnel release with medial epicondylectomy factors influencing the outcome. J Hand Surg Am. 1998; 23(3): 483-491. 8. Papatheodorou, et al. Preliminary results of recurrent cubital tunnel syndrome treated with neurolysis and porcine extracellular matrix nerve wrap. J Hand Surg Am. 2015; 40(5): 987-992 9. Lin, et al. Systematic Review and Meta-Analysis on Incidence of Altered Sensation of Mandibular Implant Surgery - PLoS One. 2016; 11(4): e0154082. 10. Hussaini. Procedure frequency in the jaws related to implant location. Dent Oral Craniofac Res. 2016; 2(2): 230-233. 11. Nguyen, et al. Risk factors for permanent injury of inferior alveolar and lingual nerves during third molar surgery. J Oral Maxillofac Surg. 2014; 72(12): 2394-2401. 12. Cheung, et al. Incidence of neurosensory deficits and recovery after lower third molar surgery: a prospective clinical study of 4338 cases. Int J Oral Maxillofac Surg. 2010; 39(4): 320–326. 13. Dental Implants Market (Product - Endosteal Implants, Subperiosteal Implants, Transosteal Implants, Intramucosal Implants; Material - Titanium Implants, Zirconium Implants; End User - Hospitals, Dental Clinics, and Academic & Research Institutes) - Global Industry Analysis, Size, Share, Growth, Trends, and Forecast 2017 – 2025. https://www.transparencymarketresearch.com/dental-implants-market.html 14. Cha, et al. Frequency of bone graft in implant surgery. Maxillofac Plast and Reconstr Surg. 2016; 38(1): 19. 15. Miloro, M (ed). Trigeminal Nerve Injuries. Springer; 2013. 16. Pogrel et al. Permanent nerve involvement resulting: From inferior alveolar nerve blocks. J Am Dent Assoc. 2000; 131(7): 901-907. 17. Agbaje, et al. Systematic review of the incidence of inferior alveolar nerve injury in bilateral sagittal split osteotomy and the assessment of neurosensory disturbances. Int. J Oral Maxillofac. Surg. 2015; 44(4): 447-451. 18. ASPS 2017– Plastic Surgery Statistics Report. www.plasticsurgery.org/documents/News/Statistics/2017/plastic-surgery-statistics-full-report-2017.pdf 19. Rappaport, et al. Clinical utilization and complications of sural nerve biopsy. Am J Surg. 1993; 166(3): 252-256. 20. Weber, et al. A randomized prospective study of polyglycolic acid conduits for digital nerve reconstruction in humans. Plast Reconstr Surg. 2000; 106(5): 1036-1045. 21. Wangensteen, et al. Collagen tube conduits in peripheral nerve repair: A retrospective analysis. Hand. 2010; 5(3): 273-277. 22. Data on file at Axogen 23. Karabekmez, et al. Early clinical outcomes with the use of decellularized nerve allograft for repair of sensory defects within the hand. Hand. 2009; 4(3): 245-249. 24. Boeckstyns, et al. Collagen conduit versus microsurgical neurorrhaphy: 2-year follow-up of a prospective, blinded clinical and electrophysiological multicenter randomized, controlled trial. J hand Surg Am. 2013; 38(12): 2405-2411. 25. Brushart, et al. Selective reinnervation of distal motor stumps by peripheral motor axons. Exp Neurol. 1987; 97(2): 289-300. 26. Schmidhammer, et al. Alleviated tension at the repair site enhances functional regeneration: The effect of full range of motion mobilization on the regeneration of peripheral nerves--histologic, electrophysiologic, and functional results in a rat model. J Trauma. 2004; 56(3): 571-584. 27. Tang, et al. The optimal number and location of sutures in conduit-assisted primary digital nerve repair. J Hand Surg Eur Vol. 2018; 43(6): 621-625. 28. Data on file at Axogen 29. Badylak, et al. Small intestinal submucosa: A substrate for in vitro cell growth. J Biomater Sci Polym Ed. 1998; 9(8): 863-878. 30. Hodde, et al. Effects of sterilization on an extracellular matrix scaffold: Part II. Bioactivity and matrix interaction. J Mater Sci Mater Med. 2007; 18(4): 545-550. 31. Nihsen, et al. Bioactivity of small intestinal submucosa and oxidized regenerated cellulose/collagen. Adv Skin Wound Care. 2008; 21(10): 479-486. 32. Hodde, et al. Vascular endothelial growth factor in porcine-derived extracellular matrix. Endothelium. 2001; 8(1): 11-24. 33. Data on file at Axogen 34. Kokkalis, et al. Assessment of processed porcine extracellular matrix as a protective barrier in a rabbit nerve wrap model. J Recon MicroSurg. 2011; 27(1): 19-28. 35. Data on file at Axogen 36. Data on file at Axogen revolutionizing the science of nerve repair™ |
|
38 Footnotes 37. Mitchell A Pet 1, Jason H Ko, Janna L Friedly, Douglas G SmithTraction Neurectomy for Treatment of Painful Residual Limb Neuroma in Lower Extremity Amputees J Orthop Trauma. 29 (9), e321-5 Sep 2015. 38. Laborde K, et al. Results of surgical treatment of painful neuromas of the hand. The Journal of Hand Surgery. March 1981;7(2):190-193. 39. Galeano M, et al. A free vein graft cap influences neuroma formation after nerve transection. Microsurgery. 2009;29(7):568-572. 40. Stokvis A. Surgical management of painful neuromas. Rotterdam, The Netherlands: Optima Grafische Communicatie; 2010. 41. Lin E, et al. Local administration of norephinephrine in the stump evokes dose-dependent pain in amputees. Clin J Pain. 2006;22(5):482-486. 42. O’Reilly MA, et al. Neuromas as the cause of pain in the residual limbs of amputees. An ultrasound study. Clin Radiology. May 1-6, 2016. 43. Rajput K, et al. Painful neuromas. The Clinical Journal of Pain. 2012;28(7):639-645 44. Gruber H, et al. Practical experience with sonographically guided phenol instillation of stump neuroma: predictors of effects, success, and outcome. Am J Roentgenol. 2008;190(5):1263-1269. 45. Fallat L. Cryosurgery or sclerosing injections: which is better for neuromas. Podiatry Today. 2004;17(6):58-66. 46. Bradley MD. Plantar neuroma: analysis of results following surgical excision in 145 patients. South Med J. 1976;69:853-845. 47. Kehoe S, et al. FDA-approved guidance conduits and wraps for peripheral nerve injury: A review of materials and efficacy. Injury. 2012;43:553-572. Biomaterials. 2001 Oct;22(19):2653-9. 48. Record RD1, Hillegonds D, Simmons C, Tullius R, Rickey FA, Elmore D, Badylak SF. In vivo degradation of 14C-labeled small intestinal submucosa (SIS) when used for urinary bladder repair. 49. Safa B, Power D, Liu A, Thayer WP, et al. A Propensity Matched Cohort Study on Outcomes from Processed Nerve Allograft and Nerve Autograft in Upper Extremity Nerve Repairs. In: The 75th Annual Meeting of the ASSH. Virtual Annual Meeting, October 1-2, 2020. 50. Sallam AA, El-Deeb MS, Imam MA. Nerve Transfer Versus Nerve Graft for Reconstruction of High Ulnar Nerve Injuries. J Hand Surg Am. 2017 Apr;42(4):265-273 51. Roganovic Z, Pavlicevic G. Difference in recovery potential of peripheral nerves after graft repairs. Neurosurgery. 2006 Sep;59(3):621-33; discussion 621-33. 52. Frykman G, Gramyk K. Results of nerve grafting. In: Gelberman R, ed. Operative nerve repair and reconstruction. Philadelphia: JB Lippincott, 1991:553–567. 53. Vastamäki M, Kallio PK, Solonen KA. The results of secondary microsurgical repair of ulnar nerve injury. J Hand Surg Br. 1993 Jun;18(3):323-6. 54. Kallio PK, Vastamäki M, Solonen KA. The results of secondary microsurgical repair of radial nerve in 33 patients. J Hand Surg Br. 1993 Jun;18(3):320-2. 55. Styron JF, Thompson AK, Park LI, Watson GJ. Nerve Repair Hospital Index Procedure Costs – Allograft vs. Autograft Repair Type. In: The 75th Annual Meeting of the ASSH. Virtual Annual Meeting, October 1-2, 2020. 56. U.S. Centers for Medicare and Medicaid Services, Medicare Claims standard analytic file. 2018. 57. Data on file at Axogen. revolutionizing the science of nerve repair™ Avance Nerve Graft, Axoguard Nerve Protector, Axoguard Nerve Connector, Axoguard Nerve Cap, Avive Soft Tissue Membrane, RANGER, MATCH, RECON, REPOSE, Sensation-NOW, revolutionizing the science of nerve repair, and their logos are trademarks of Axogen Corporation. Axoguard Nerve Connector and Axoguard Nerve Protector are manufactured in the United States by Cook Biotech Incorporated, West Lafayette, Indiana, and are distributed exclusively by Axogen Corporation. LB-0588 |